Vitamin D deficiency is a common concern among patients with obesity due to factors such as reduced sun exposure, dietary insufficiency, and altered metabolism. Identifying the best vitamin D test for this population is crucial, as standard assays may yield inaccurate results due to the unique distribution of vitamin D in adipose tissue. The total 25-hydroxyvitamin D (25(OH)D) test, which measures both free and bound forms, is often recommended, but emerging evidence suggests that assessing bioavailable or free 25(OH)D may provide a more accurate reflection of vitamin D status in obese individuals. Understanding the limitations and strengths of these tests is essential for clinicians to ensure appropriate diagnosis and management of vitamin D deficiency in this high-risk group.
| Characteristics | Values |
|---|---|
| Test Type | 25-Hydroxyvitamin D [25(OH)D] test (considered the gold standard) |
| Preferred Method | Liquid chromatography-tandem mass spectrometry (LC-MS/MS) |
| Reason for Preference | High accuracy, specificity, and ability to differentiate D₂ and D₃ forms |
| Alternative Methods | Automated immunoassays (less accurate in obesity due to cross-reactivity) |
| Sample Type | Serum or plasma |
| Reference Range | Varies by lab, but generally: Sufficient ≥ 20 ng/mL, Insufficient < 20 ng/mL |
| Adjustments for Obesity | Higher doses of vitamin D supplementation may be needed due to sequestration in adipose tissue |
| Frequency of Testing | Baseline and follow-up testing recommended for obese patients |
| Considerations | Volume of distribution (VD) of vitamin D is higher in obese individuals |
| Limitations of Standard Tests | Immunoassays may overestimate 25(OH)D levels in obesity |
| Clinical Relevance | Obese patients often require 2-3 times the standard vitamin D dose |
| Monitoring | Regular monitoring due to higher risk of vitamin D deficiency in obesity |
| Cost | LC-MS/MS is more expensive but more reliable |
| Availability | LC-MS/MS may not be widely available in all labs |
| Patient Factors | BMI, fat mass, and comorbidities influence vitamin D status |
Explore related products


![Vitamin D Test Kit at Home [2 Tests] for Testing Vitamin D Deficiency](https://m.media-amazon.com/images/I/61keZmSELiL._AC_UL320_.jpg)



What You'll Learn
![]()
25-Hydroxyvitamin D Test Accuracy
The 25-Hydroxyvitamin D (25(OH)D) test is widely recognized as the gold standard for assessing vitamin D status in the general population. However, its accuracy in patients with obesity is a subject of growing interest due to the unique physiological challenges this group presents. Obesity alters vitamin D metabolism, as the vitamin becomes sequestered in adipose tissue, potentially leading to lower circulating levels despite adequate storage. This phenomenon raises questions about whether standard 25(OH)D thresholds accurately reflect vitamin D sufficiency in individuals with higher body mass indices (BMIs).
Analytically, the 25(OH)D test measures both vitamin D₂ and D₃ metabolites, providing a comprehensive snapshot of total body stores. Yet, in obesity, the test may underestimate bioavailable vitamin D, as a larger proportion remains trapped in fat tissue. Studies suggest that free or bioavailable 25(OH)D, which accounts for the fraction not bound to proteins, might be a more accurate marker in this population. For instance, a 2019 study in *The Journal of Clinical Endocrinology & Metabolism* found that free 25(OH)D levels correlated more closely with bone health markers in obese individuals than total 25(OH)D.
Instructively, healthcare providers should consider BMI-specific reference ranges when interpreting 25(OH)D results for obese patients. Current guidelines often recommend a target 25(OH)D level of 20–50 ng/mL for the general population, but obese individuals may require higher levels (e.g., 30–60 ng/mL) to achieve similar physiological effects. Additionally, dosing vitamin D supplements in obesity typically requires higher amounts—up to 2–3 times the standard dose of 600–800 IU/day—to achieve target levels due to increased sequestration and reduced bioavailability.
Persuasively, while the 25(OH)D test remains the most practical tool for assessing vitamin D status, its limitations in obesity highlight the need for adjunctive measures. Combining 25(OH)D testing with assessments of parathyroid hormone (PTH) levels or bone turnover markers can provide a more nuanced understanding of vitamin D adequacy. For example, elevated PTH in the presence of "normal" 25(OH)D levels may indicate functional deficiency in obese patients.
Comparatively, newer assays for free 25(OH)D or vitamin D-binding protein (DBP) levels offer promising alternatives but are not yet widely available or standardized. Until these methods become mainstream, clinicians must rely on the 25(OH)D test while acknowledging its limitations. Practical tips include monitoring obese patients more frequently (e.g., every 3–6 months) and individualizing treatment based on clinical response rather than relying solely on lab values.
In conclusion, the 25(OH)D test remains the cornerstone of vitamin D assessment, even in obesity, but its interpretation requires careful consideration of BMI-related factors. By integrating clinical context, adjusting dosing strategies, and exploring emerging biomarkers, healthcare providers can optimize vitamin D management in this challenging population.
Optimal Timing for Vitamin C Serum Application: A Skincare Guide
You may want to see also
Explore related products





![]()
Bioavailable vs. Total Vitamin D
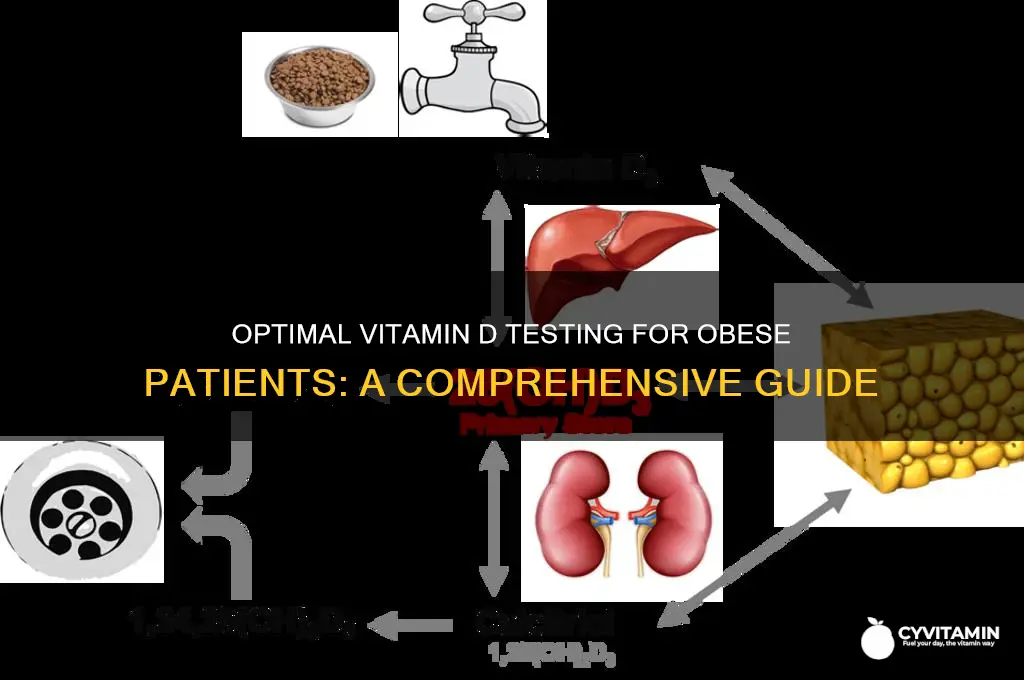
Obesity complicates vitamin D assessment because it alters how the body stores and releases this fat-soluble nutrient. Standard tests measure total vitamin D, which includes both bound and free fractions. However, bioavailable vitamin D—the unbound, metabolically active portion—may be a more accurate indicator of functional status in obese individuals. Understanding this distinction is crucial for interpreting test results and tailoring supplementation strategies.
Consider the mechanics: in obesity, vitamin D becomes sequestered in adipose tissue, reducing its circulation in the bloodstream. This can lead to misleadingly low total vitamin D levels, even when bioavailable levels are sufficient. Conversely, high total levels might not translate to adequate bioavailability if most of the vitamin D remains trapped in fat stores. A 2019 study in *The Journal of Clinical Endocrinology & Metabolism* found that obese individuals had significantly lower bioavailable vitamin D compared to their non-obese counterparts, despite similar total levels.
Testing for bioavailable vitamin D involves measuring free 25-hydroxyvitamin D or calculating it using formulas that account for vitamin D-binding protein (DBP) concentrations. While not yet standard practice, this approach offers a more precise assessment of vitamin D’s active form. For example, an obese patient with a total 25(OH)D level of 30 ng/mL (considered adequate) might have a low free 25(OH)D level, indicating a functional deficiency. Clinicians should consider this discrepancy when deciding on supplementation, especially since obese individuals often require higher doses—up to 2–3 times the standard 600–800 IU/day—to achieve target levels.
Practical tips for healthcare providers: first, recognize that BMI is a key factor in test interpretation. Second, advocate for bioavailable vitamin D testing when total levels are ambiguous or when patients remain symptomatic despite supplementation. Third, monitor response to therapy closely, as obese patients may require longer treatment durations. Finally, emphasize lifestyle modifications, such as weight loss and increased sun exposure, to enhance vitamin D bioavailability naturally.
In conclusion, while total vitamin D testing remains the norm, bioavailable vitamin D provides a more nuanced understanding of deficiency in obese patients. Adopting this approach can lead to more effective treatment plans, ensuring that supplementation addresses the unique metabolic challenges of this population. As research evolves, bioavailable testing may become the gold standard for obesity-related vitamin D assessment.
Gummies vs. Pills: Which Vitamin Delivery Method is Best?
You may want to see also
Explore related products






![]()
Obesity-Related Vitamin D Deficiency
Vitamin D deficiency is disproportionately prevalent in individuals with obesity, a phenomenon linked to altered metabolism, sequestration in adipose tissue, and reduced bioavailability. The standard 25-hydroxyvitamin D (25(OH)D) blood test remains the gold standard for assessing deficiency, but its interpretation in obesity requires nuance. Studies show that individuals with obesity often have lower serum 25(OH)D levels despite similar sun exposure or dietary intake compared to their non-obese counterparts. This discrepancy arises because vitamin D, a fat-soluble vitamin, becomes trapped in adipose tissue, limiting its release into circulation. Consequently, relying solely on serum 25(OH)D levels may underestimate the functional vitamin D status in this population.
When testing for vitamin D deficiency in patients with obesity, clinicians should consider the patient’s body mass index (BMI) and total body fat percentage. Research suggests that free or bioavailable 25(OH)D, which represents the unbound and metabolically active fraction of vitamin D, may be a more accurate marker in this context. However, measuring free 25(OH)D is not yet widely available or standardized, making it impractical for routine clinical use. Instead, some experts recommend adjusting supplementation dosages based on weight or BMI. For instance, individuals with obesity may require 2–3 times the standard dose (600–800 IU/day) to achieve optimal serum levels, often ranging from 2,000 to 4,000 IU/day or higher under medical supervision.
A comparative analysis of testing methods reveals that while 25(OH)D remains the primary test, its limitations in obesity highlight the need for a more comprehensive approach. Emerging biomarkers, such as vitamin D-binding protein (DBP) levels, could offer additional insights, as DBP plays a critical role in vitamin D transport and bioavailability. However, until these markers are validated and standardized, clinicians must rely on clinical judgment and individualized treatment plans. Monitoring patients with obesity for symptoms of deficiency, such as bone pain, muscle weakness, or fatigue, is equally important, as these may manifest despite seemingly adequate serum 25(OH)D levels.
Practically, addressing obesity-related vitamin D deficiency involves a two-pronged strategy: optimizing testing and tailoring supplementation. For patients with a BMI ≥30 kg/m², starting with a higher baseline dose of vitamin D and retesting after 8–12 weeks is advisable. Encouraging lifestyle modifications, such as weight loss and increased physical activity, can also improve vitamin D status by reducing adipose sequestration and enhancing overall metabolic health. Finally, clinicians should educate patients about the interplay between obesity and vitamin D, emphasizing that deficiency is not merely a matter of insufficient intake but a complex metabolic issue requiring targeted intervention.
Boosting Recovery: Top Vitamins for Epstein-Barr Syndrome Support
You may want to see also
Explore related products






![]()
Test Interpretation in High BMI
Obesity complicates vitamin D testing due to its sequestration in adipose tissue, leading to lower serum concentrations despite adequate total body stores. The standard 25-hydroxyvitamin D (25(OH)D) test, while widely used, may not accurately reflect bioavailable vitamin D in this population. This discrepancy arises because vitamin D binds to both vitamin D-binding protein (DBP) and albumin, but only the free or albumin-bound fractions are metabolically active. In individuals with high BMI, increased volume of distribution and altered DBP levels can skew results, often suggesting deficiency when none exists.
Interpreting 25(OH)D levels in obese patients requires a nuanced approach. A threshold of 20 ng/mL is commonly used to define deficiency, but this may overestimate prevalence in obesity. Research suggests that obese individuals with levels above 16 ng/mL may still have sufficient vitamin D for bone health, as adipose tissue acts as a reservoir. However, supplementation based solely on 25(OH)D levels can lead to excessive dosing, increasing the risk of hypercalcemia. Clinicians should consider free or bioavailable vitamin D assays, though these are not yet standardized and may not be widely available.
A practical strategy involves correlating 25(OH)D levels with clinical symptoms and risk factors. Obese patients with bone pain, fractures, or secondary hyperparathyroidism warrant closer scrutiny, even if their 25(OH)D is marginally low. Supplementation should start at a lower dose, such as 1000–2000 IU/day, with retesting after 3 months. For those with severe deficiency (<10 ng/mL), a loading dose of 50,000 IU weekly for 8 weeks may be considered, followed by maintenance therapy. Monitoring calcium levels is essential to avoid toxicity, particularly in older adults or those with renal impairment.
Comparatively, the free 25(OH)D test offers a more accurate assessment of bioavailable vitamin D but is not yet routine. Studies show that free 25(OH)D correlates better with parathyroid hormone levels in obese individuals, providing a more reliable marker of functional deficiency. However, its cost and limited availability restrict widespread use. Until more accessible methods are developed, clinicians must rely on clinical judgment, adjusting interpretation and treatment based on individual patient factors rather than 25(OH)D levels alone.
In conclusion, interpreting vitamin D tests in high-BMI patients demands a tailored approach. Blindly applying standard thresholds risks misdiagnosis and overtreatment. By integrating clinical context, considering alternative assays, and adopting conservative supplementation strategies, healthcare providers can optimize vitamin D management in this challenging population. Future research into adipose tissue dynamics and bioavailable vitamin D will further refine these practices.
Boost Sleep Quality: Top Vitamins to Take Before Bed
You may want to see also
Explore related products






![]()
Alternative Testing Methods
Obesity complicates vitamin D testing due to its volumetric distribution in adipose tissue, which can dilute serum levels and lead to inaccurate results. Standard 25-hydroxyvitamin D (25(OH)D) assays may underestimate bioavailable vitamin D in this population. Alternative testing methods aim to address this limitation by focusing on free or bioactive fractions of the vitamin. One such method is measuring free 25(OH)D, which represents the unbound, metabolically active portion not sequestered in fat tissue. This approach provides a more accurate reflection of vitamin D status in patients with obesity, as it accounts for the altered physiology of fat storage.
Another innovative technique involves assessing vitamin D-binding protein (DBP) levels alongside total 25(OH)D. DBP is responsible for transporting vitamin D in the bloodstream, and its concentration can vary independently of obesity. By calculating the bioavailable or free 25(OH)D using DBP levels, clinicians can better interpret vitamin D status in obese individuals. For instance, a patient with low total 25(OH)D but normal DBP-adjusted levels may not require supplementation, despite conventional thresholds suggesting deficiency.
A third alternative is the use of liquid chromatography-tandem mass spectrometry (LC-MS/MS) for 25(OH)D measurement. This method offers superior accuracy and precision compared to immunoassays, which are prone to cross-reactivity with vitamin D metabolites. LC-MS/MS can differentiate between 25(OH)D2 and 25(OH)D3, providing a more detailed profile of vitamin D status. For obese patients, this specificity is crucial, as it helps distinguish between dietary intake, supplementation, and endogenous production, guiding tailored treatment plans.
Finally, functional biomarkers like parathyroid hormone (PTH) and bone turnover markers can complement traditional vitamin D testing. Elevated PTH levels in the presence of low 25(OH)D suggest true deficiency, even if total levels appear borderline. Monitoring these markers can help determine the clinical relevance of vitamin D status in obese patients, ensuring that supplementation is targeted to those with demonstrable physiological impact. For example, a patient with 25(OH)D of 20 ng/mL and normal PTH may not require intervention, whereas another with the same 25(OH)D but elevated PTH would benefit from supplementation.
In practice, clinicians should consider these alternative methods when standard 25(OH)D testing yields ambiguous results in obese patients. Combining free 25(OH)D, DBP assessment, LC-MS/MS, and functional biomarkers provides a more comprehensive understanding of vitamin D status, enabling precise and personalized care. While these methods may require specialized equipment or additional costs, their value lies in avoiding unnecessary supplementation and identifying true deficiency in a population where conventional testing often falls short.
Top Vitamins for Perimenopause Relief: Essential Supplements Guide
You may want to see also
Frequently asked questions
The best vitamin D test for patients with obesity is the 25-hydroxyvitamin D (25(OH)D) blood test, as it accurately measures the total vitamin D levels in the body, including both dietary and sunlight-derived sources.
The 25-hydroxyvitamin D test is preferred because vitamin D is fat-soluble and can be sequestered in adipose tissue in obese individuals, leading to lower circulating levels. This test provides a reliable assessment of bioavailable vitamin D.
Yes, obese patients may require higher doses of vitamin D supplementation due to sequestration in fat tissue. Additionally, healthcare providers should interpret test results cautiously, as obese individuals often have lower serum 25(OH)D levels despite adequate total body stores.